The acromioclavicular (AC) joint is where the collar bone (clavicle) meets a small, forward-jutting arch of the shoulder blade (acromion). If you follow your collarbone to where it meets the front of your shoulder, you will find your AC joint.
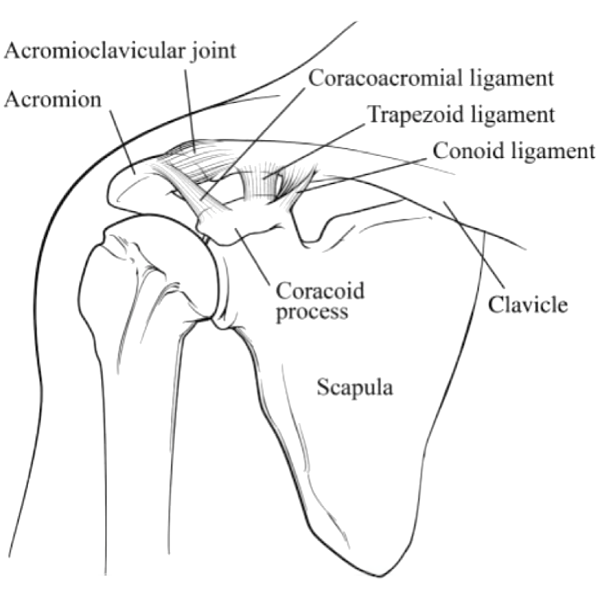
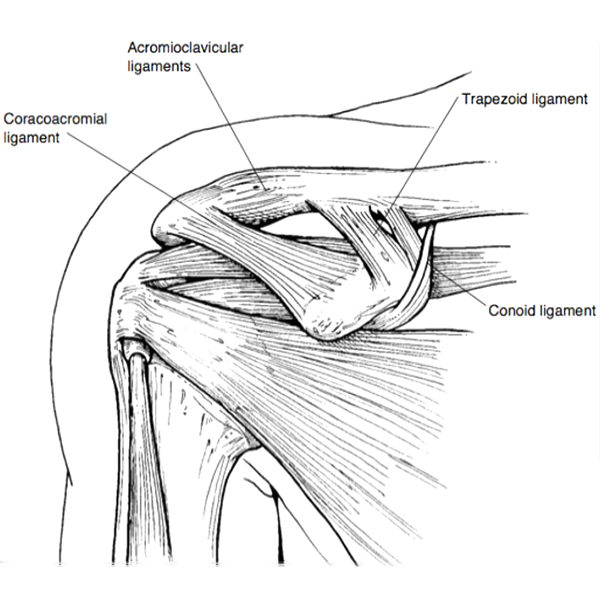
Two main ligaments hold these bones together:
- The AC ligament connects the acromion and the clavicle and stops the AC joint from coming apart.
- The coracoclavicular (CC) ligament connects the clavicle and the shoulder blade (scapula) and stabilizes the AC joint.
In an AC separation, one or both of these ligaments may be injured.
This type of injury is especially common with cyclists who fall forward onto an outstretched arm.
Symptoms
The symptoms of an AC joint separation vary by the severity of the injury.
- Type I: The AC ligament is partially torn (sprained). There is pain and mild swelling.
- Type II: The AC ligament is fully torn, and the CC ligament is sprained. There is pain and significant swelling.
- Type III: Both the AC and CC ligaments are fully torn. There is significant pain and swelling.
- Type IV, V, VI: More severe injuries to the AC and CC ligaments that require surgery.
With the more severe types of injury, there is often a bump where the clavicle becomes more prominent because it has lost its anchor to the shoulder blade. The pain usually subsides within a few weeks, but the deformity may never go away. A deformity alone, without pain, is not a good reason to have surgery.
With a very forceful trauma, the clavicle can break through the muscle layer of the deltoid and trapezius and can be seen under the skin.
Causes
The AC joint can get injured—or “separated”—in a fall or from a blow to the shoulder. This type of injury is especially common with cyclists who fall forward onto an outstretched arm, as well as in contact-sport athletes, like football players.
Diagnosis
An AC joint separation is easy to spot when it causes a visible deformity. Otherwise, the location of pain and x-rays can help confirm the diagnosis.
Nonsurgical treatment options
Most cases of AC separation are treated without surgery. Treatment varies by type and may include:
- Rest or activity modification
- Use of ice packs to relieve swelling and pain
- Pain medication (e.g., acetaminophen or ibuprofen)
- Immobilization in a sling
- Type I AC injuries may require a sling for a few days
- Type II AC injuries may require a sling for three to seven days
- Type III AC injuries may require a sling for three to four weeks
- Physical therapy
Recovery times for AC separation also varies by type:
- Type I AC injuries may require three days to two weeks to heal
- Type II AC injuries may require two to four weeks to heal
- Type III AC injuries may require six to twelve weeks to heal
For most patients with type I–III AC joint injuries, surgery is advised only if their symptoms do not improve to the level that they desire. Surgery is generally recommended for type IV-VI AC injuries.
A type IV AC joint injury is when the clavicle is displaced backward through the trapezius muscle; this occurs when the injury to the point of the shoulder causes the scapula to rotate forward and inward towards the chest, causing the clavicle to push through the posterior AC joint capsule and then the trapezius.
A type V AC joint injury occurs when the scapula is severely depressed downward, rupturing the AC and CC ligaments, then progressing through the deltotrapezial fascia. The trapezius loses its ability to shrug the shoulder upwards.
A type VI AC joint injury, the rarest of all types, occurs with the scapula being displaced posterior, allowing for the clavicle to become lodged underneath the coracoid of the scapula. Surgery is recommended in these injuries to restore the relationship between the clavicle and the scapula. Without surgical repair, permanent limitation of function and persistent pain with activity is likely.
When these injuries occur, especially with Types I, II, III, and V, initial treatment is usually nonsurgical, including rest, ice, sling for supporting arm as needed, and medication for discomfort. If the results of the early conservative treatment are not successful, the good news is that surgery three or more months after the injury typically has the same level of success, in terms of return to preinjury function, as surgery that is done right away. However, the surgeon has to include reconstruction of the ligaments with a tendon graft with delayed surgery. So it’s ok to wait. By waiting to see if the shoulder improves without surgery, only a few patients will end up actually needing an operation.
How surgery is performed
AC joint reconstruction surgery uses a tendon graft to rebuild the AC and CC ligaments. It also uses a powerful synthetic tape to hold the repair together while the soft tissues such as the graft progress through the healing process. And, as the tape is integrated into your healing tissue, it helps to reinforce the final surgical reconstruction.
Most of the procedure is performed arthroscopically through small incisions around the shoulder. In addition, the arthroscope allows an inspection of the shoulder (glenohumeral) joint, where up to 15-20% of patients may have additional injuries.
After removing damaged tissue from where the ligaments attach between the clavicle and the coracoid, a synthetic tape is passed between the clavicle and the coracoid. This is followed by the passing of a tendon, usually a hamstring tendon graft, around the coracoid and the clavicle.
Once this is all completed arthroscopically, a small incision is made on the top of the shoulder to complete the stabilization of the coracoid (scapula) to the clavicle with the synthetic tape, secure the tendon graft, and repair or reconstruct the AC ligament. The final step is repairing the strong tissue between the deltoid and the trapezius muscles to ensure the trapezius heals to the scapula.
The entire weight of the arm pulls downward on the surgical site. Despite the strength of this surgical procedure, additional support to the arm and shoulder is necessary to help counter gravity.
Therefore, it is essential that your arm and shoulder are supported in a sling and pillow brace, or in some cases a firm gunslinger orthosis, whenever you are standing or sitting. This is commonly used when a patient has failed to achieve the desired outcome with prior surgery on the AC joint and revision surgery is indicated. Furthermore, the brace needs to be in place at night when you are sleeping to avoid inadvertent pressure on the reconstruction or use of the arm. The brace is a necessary part of the success of this surgery.
The operation is typically performed at an ambulatory surgery center on an outpatient basis. Again, more than two-thirds of the procedure is performed arthroscopically to minimize injury to the normal healthy tissues of the shoulder.
Before you leave to recover at home, we will review your postoperative plan, including the need for wearing the brace, the first follow-up visit in seven to ten days, and the plan to start supervised physical therapy approximately six weeks after the surgery.
If you are a cyclist, you can get back on the road with your bike at three months post-op and on trails at around six months.

Recovery time
You will go home the same day as your surgery to recover in the comfort of your home. You will need to wear a sling and pillow brace (Slingshot or Ultrasling) for six weeks after surgery. Sutures are taken out one week after surgery. Dr. Romeo will give you specific instructions for post-op pain management. Cold therapy is very helpful to control the swelling and pain after surgery.
After six weeks, you will begin a course of physical therapy to build flexibility in the shoulder, and then gradually work toward a strengthening program. You will need to move your shoulder, wrist, fingers, and elbow every day to prevent muscle stiffness and ensure the joint does not become locked into a narrow range of motion.
By the third month, you will be able to engage in most of your normal daily activities, however, it often takes another three months or more to get your strength back for strenuous activities or recreational sports.
If you are a cyclist, you can get back on the road with your bike at three months post-op and on trails around six months. No surgery or brace can prevent this injury from happening again if you have an accident on your bike and land on your shoulder, so please be careful.
Results
Fortunately, with the advanced techniques we use—which include an internal brace with synthetic tape combined with a tendon graft—the procedure is highly effective at stabilizing the AC joint, restoring flexibility and range of motion to the joint, and allows for an advanced strengthening program over time. In fact, an estimated 90% of patients are able to resume the same brisk tempo of physical activity they engaged in before the injury.
The surgery also has a high patient satisfaction rate. In addition to treating your pain, the procedure also has an aesthetic component: it eliminates most of the visible bump seen on top of the shoulder, although you may continue to see a small step-off between the collar bone and the shoulder blade. This is common even on shoulders that have not been injured because the end of the clavicle has a tendency to widen and increase in size over our lifetime. And, don’t forget, you will have a permanent scar from the incision—although this will blend in nicely with your skin and be easily covered with most shirts and blouses.
FAQs
Can I take a cortisone shot to get back in the game more quickly?
In high-level college or professional athletes that may want to return quickly to their sport during the competitive season, corticosteroid injections into the AC joint can help alleviate swelling and pain, allowing the athlete to compete. However, this may expose the joint to more injury, and therefore this treatment is used very cautiously. More recently, platelets from your blood, or platelet-rich plasma, have been injected into the injured AC joint to help accelerate the healing process and return to activities.
